

Introduction
P-2001, a randomized phase 2 trial (NCT02610777), investigated the efficacy and safety of pevonedistat (P), the first small-molecule inhibitor of the NEDD8-activating enzyme, in combination with azacitidine (A) versus A alone in patients (pts) with higher-risk (Revised International Prognostic Scoring System risk >3, including intermediate [≥5% blasts], high, or very high risk) myelodysplastic syndromes (MDS)/chronic myelomonocytic leukemia (CMML), or low-blast acute myeloid leukemia (LB AML) naïve to hypomethylating agents. The P-2001 trial recently demonstrated median event-free survival of 21.0 vs 16.6 months (HR=0.665; P = .076), and overall response rates (complete remission [CR] + CR with incomplete blood count recovery [CRi] + partial response [PR] + hematologic improvement [HI]) of 71% (n=39/55) vs 60% (n=32/53) with P+A compared with A, respectively. Management of MDS can significantly impact quality of life, and measures of high-symptom burden have been associated with worse clinical outcomes. We set out to explore patient-reported outcomes (PRO) as an exploratory endpoint in the study.
Methods
The study randomized 120 pts (1:1) to receive P+A or A alone in 28-day treatment cycles. The European Organisation for Research and Treatment of Cancer (EORTC) quality of life questionnaire - core 30 items (QLQ-C30) was administered at the first day of each cycle, at the end of treatment (EOT) visit and post-EOT visits. Physical functioning (PF), fatigue (FA), dyspnea (DY) and global health status/quality of life (QL) were identified as key PRO concepts that deserved specific attention in this population. Analyses were carried out to explore the PRO data: description of available PRO data, longitudinal analyses of change in the key PRO scores with repeated measurement mixed models (RMMM), including comparison between treatment arms, and descriptive analysis of the key PRO scores after clinical response depending on the type of response (PR, CR, CRi, or HI), and before and after transformation to AML for pts with higher-risk MDS, independently from the treatment received.
Results
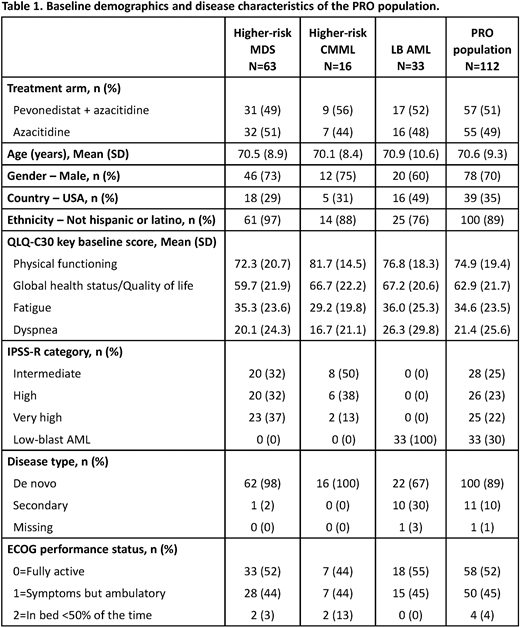
There were 112 pts in the PRO population (defined as all pts with a PRO assessment at baseline and at least 1 post-baseline); baseline demographics and disease characteristics are presented in Table 1. At least 90% of pts in the study had a PRO available at each cycle. As expected, the amount of available PRO data decreased over the study due to progression, death, or study discontinuations. The RMMMs of the PRO population did not show any statistically significant difference in the change over time in key QLQ-C30 scores (PF, QL, FA, and DY) between P+A versus A alone. Pts who experienced CR (P+A, 40%; A, 29%) showed a nonsignificant improvement in PF and QL, as well as a nonsignificant decrease of FA after CR than at baseline; no differences were noted in DY. Pts for whom best response was PR had less improvement in the key PROs than pts with CR, and those with HI did not show improvement compared with baseline. Among the 12 pts with higher-risk MDS/CMML progressing to AML during the study with available PRO data (P+A, n=4; A, n=8), 6 showed worsening in PF score (vs 2 improving), 6 showed worsening in QL score (vs 1 improving), 7 showed worsening in FA score (vs 1 improving), and 7 showed worsening in DY score (vs none improving).
Conclusions
Measurement of QL and symptom burden are integral clinical endpoints in assessing new treatments in higher-risk MDS/CMML and LB AML. There was no evidence to suggest that the addition of P to A led to change in the key PROs identified: QL, PF, FA and DY. Achievement of CR was associated with higher PRO scores compared with baseline independently of the treatment received, and progression to AML was associated with worsening QL scores. Additional analyses are planned with the P-2001 PRO data to further explore the impact of P on PROs by evaluating the impact of dropout during the study, comparing findings according to treatment arm, and better understanding the possible effect of adverse events on PROs.
Zeidner:AbbVie: Honoraria, Other: Independent Review Committee; Agios: Honoraria; AROG: Research Funding; AsystBio Laboratories: Consultancy; Sumitomo Dainippon Pharma Oncology, Inc.: Research Funding; Genentech: Honoraria; Daiichi Sankyo: Honoraria; Celgene: Consultancy, Honoraria, Research Funding; Forty-Seven: Other: Travel Reimbursement, Research Funding; Merck: Research Funding; Pfizer: Honoraria; Takeda: Consultancy, Honoraria, Other: Travel Reimbursement, Research Funding. Mazerolle:Takeda Pharmaceutical Company: Other: Granted research funding to Modus Outcomes, my employer; Modus Outcomes: Current Employment. Bell:Millennium Pharmaceuticals, Inc.: Current Employment. Cain:Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited: Current Employment. Faller:Phoenicia Biosciences: Consultancy, Current equity holder in private company, Membership on an entity's Board of Directors or advisory committees, Patents & Royalties; Viracta Therapeutics: Consultancy, Current equity holder in private company, Membership on an entity's Board of Directors or advisory committees, Patents & Royalties; Millennium Pharmaceuticals Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited: Current Employment; Briacell Therapeutics: Consultancy, Current equity holder in private company, Membership on an entity's Board of Directors or advisory committees, Patents & Royalties. Dalal:Millennium Pharmaceuticals Inc, a wholly owned subsidiary of Takeda Pharmaceutical International Company, Cambridge, MA: Current Employment, Current equity holder in private company. Regnault:Modus Outcomes: Current Employment. Fram:Teva: Current equity holder in publicly-traded company; Baxter: Current equity holder in publicly-traded company; Gilead: Current equity holder in publicly-traded company; Pfizer: Current equity holder in publicly-traded company; Bristol Myers Squibb: Current equity holder in publicly-traded company; Takeda: Current equity holder in publicly-traded company; Vertex Phamaceuticals: Patents & Royalties: Patent 10/728,114; Takeda Pharmaceuticals Intl. Co.: Consultancy, Current Employment; BeyondSpring Pharmaceuticals Inc.: Consultancy.
Pevonedistat is the first small molecule inhibitor of the neural precursor cell expressed, developmentally downregulated 8 (NEDD8)-activating enzyme (NAE)

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal